From 1993 until 2011 it worked for Bill Clinton and the gay component of the military. . .
. . .the question is, will it work for my oncologist? Probably.
Will it work for me? Probably not.
I spoke to Adrian Donaldson, MS, LMHC, yesterday (April 26, 2023) about my ongoing concerns. Oh, I’m not concerned about my care — the care I get at Roswell is an overwhelming improvement over the “care” I got at Pluta/University of Rochester.

(This photo, above, shows what an incompetent doctor looks like. He appears normal enough, but that smarmy grin is a dead giveaway. His name is Ajay Dhakal. He almost killed me when he failed to recognize the deadly symptoms of typhlitis in a postchemo patient (me).) From https://www.urmc.rochester.edu/people/112361746-ajay-dhakal, August 2022
Instead, my concern is that my providers refuse to address what Dr. Dhakal did, which is driving me insane (that is, if Dr. Dhakal hasn’t done so already). Although they elicit this information during each visit, none of my visit notes ever reflect these discussions.
The one note that did (December 2022) blamed me: “The patient switched her care to Roswell because she had a bad relationship with her doctor.” When I protested this assessment, the entire reference was removed.
Their concern , which is a refusal to acknowledge this portion of my past medical history, is overriding my concern, which is watching my own caregivers distort my medical record into an instrument that protects Dr. Dhakal from himself.
My medical record should reflect what occurs between my doctor and me (it doesn’t). It should not be used to hide someone else’s incompetence (it does).
Their persistent error of omission forces me, indirectly through my own medical record, to defend a doctor who almost killed me. I required four surgeries and extensive medical care just to survive. I will live with the emotional, physical, and financial consequences for the rest of my life.
That my medical record is used to defend him is outrageous. It is also depressing.
After an emotional 17-minute phone call with Ms. Donaldson, we agreed to a strategy of “don’t ask, don’t tell.” But just how will this help me?
After a long night of deliberation, I realized the only one it will help is the provider who writes up my record. It won’t help me.
It is comforting to know that they will never ask me about “it” again, which (lucky them!) removes the need for documentation in future medical records. But my prior records remain uncorrected. During every previous visit, they asked about my prior care. They asked why I switched to Roswell.
And they consistently ignored my answer.
It’s as if my near-death didn’t happen. It’s as if it was all a bad dream.
But it did happen, and it wasn’t a dream.
It’s the elephant in the room that everyone tiptoes around. And each time that elephant is ignored, trivialized, or dismissed, it bumps into me.
Each time it bumps into me a little bit of my self-worth is chipped away.
It’s as if the elephant and I are one and the same. If the elephant isn’t recognized or acknowledged, then neither am I. If the elephant is dismissed as unimportant, then so am I.
I learned that when Holly Anderson, Director of the Breast Cancer Coalition of Rochester, demanded I “choose” to shut the f*ck up — and then promised that my world would magically improve once I did. . .but only if I did.
I fear that “don’t ask, don’t tell” is equally destructive — but only to me. It frees my providers from documenting a distressing issue, but I am condemned to keeping it a terrible secret. This causes emotional turmoil, lack of confidence, and a disastrously low self-esteem, all of which worsen the depression and anxiety.
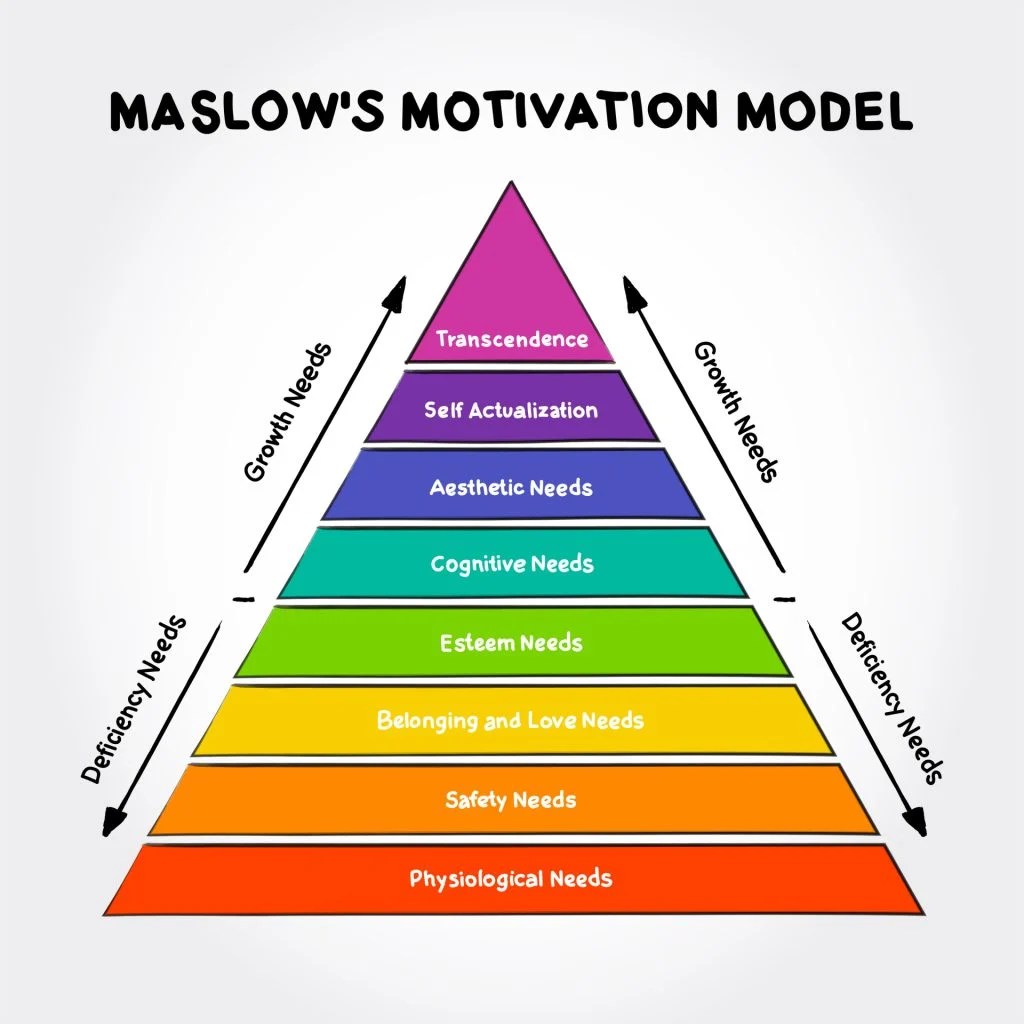
It transforms Maslow’s Hierarchy into Maslow’s Mountain and prevents me from reaching the top. It ensures that I will keep losing my step.
How long will it be before the self-esteem lessens to the point of nonexistence?
What happens then?
PART 2: Well, I’ll tell you what happens
December 29, 2023: Just as I suspected, “don’t ask / don’t tell” is working quite well for my medical providers but for me not so much.
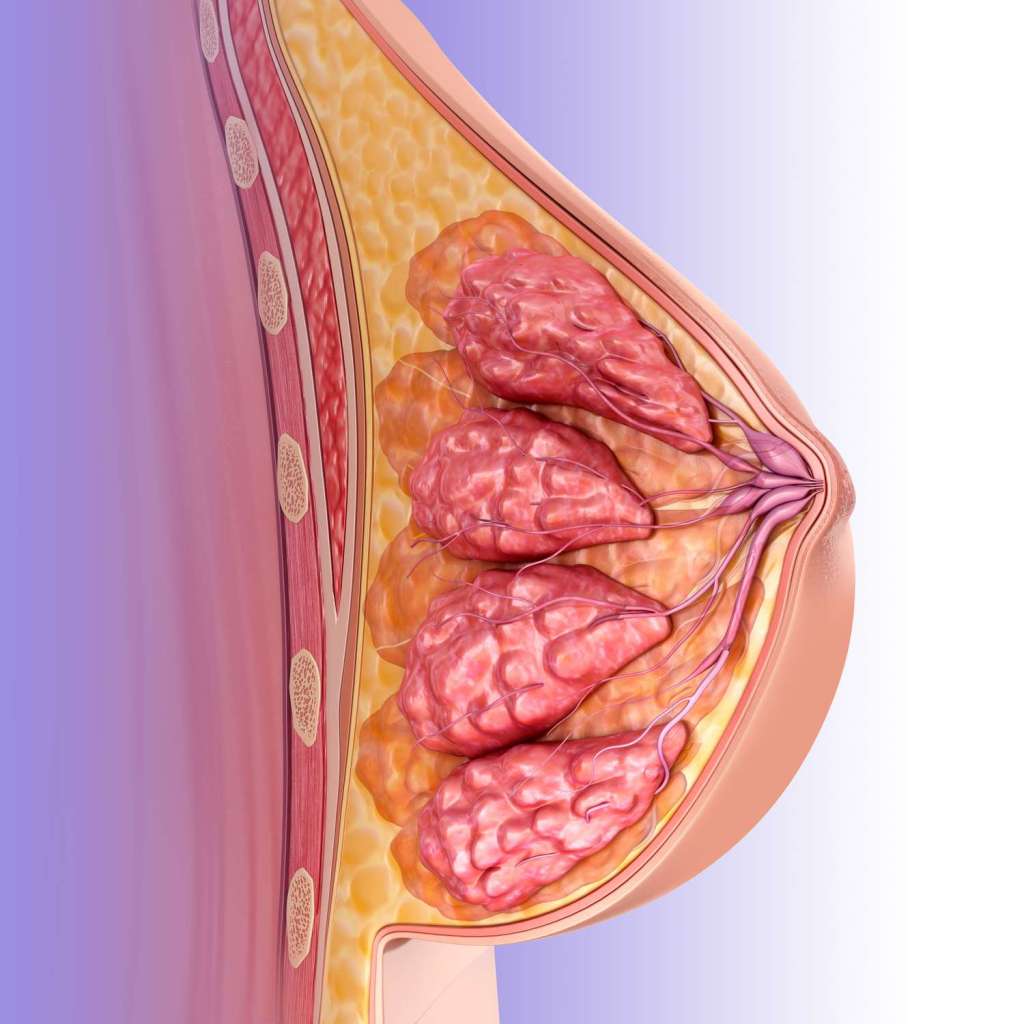
That’s me, The Breast. Notice its construction — a bunch of milk ducts, fat, and connective and muscle tissue but no brains. Thank you, Patient Advocate!
When I enter Roswell, I am no longer a person. I have been demoted to the lower life form of The Breast. The Breast used to get a thorough palpation once every three months, but at the last visit I had to request the exam. Respectful interaction, personalized care, exchange of information — you know, the “quality care” that Roswell advertises on its website — that’s reserved for persons. None of it is wasted on The Breast.
“Don’t ask / don’t tell” doesn’t stop my providers from asking me questions, but that’s okay. The Breast knows how to respond — smile and nod politely and just. don’t. tell. Oh, I am encouraged to “call us if you have any problems” but that just signals the end of the exam and that The Breast can go now. I’m not supposed to take that literally.
The Breast learned just how bad “don’t ask / don’t tell” can be when she broke the rules today (December 29, 2023) and asked questions.
What WAS I thinking!
Through MyPortal, which is the Roswell electronic charting system, I noticed that my cancer was described as “IDC-NST” (intraductal carcinoma of no special type). But my pathology report doesn’t say that. Upon examination of the surgical specimen from January 2021, two University of Rochester pathologists identified “intraductal carcinoma of no special type with medullary features.” The doctor who performed the surgery agreed with the diagnosis as did the experts at Elizabeth Wende Breast Center, who did the core biopsy. The “medullary” component is an important distinction, according to papers published by the National Institute of Health, since IDC-NST with medullary features is not the same as IDC-NST. Nor should it be confused with another cancer type, medullary carcinoma, although that is easily done since some of the studies I found on the Internet used the “medullary” terms interchangeably.
But there is a difference:
IDC-NST: https://basicmedicalkey.com/invasive-ductal-carcinoma-adenocarcinomas-of-no-special-type/
IDC-NST with medullary features: https://www.sciencedirect.com/science/article/pii/S1930043323000535
My sin was not in discovering this information. My sin was attempting to discuss it with the doctor (Shipra Gandhi, MD).
But my questions were intercepted by “the team.”

At first “the team” could not respond because they were “waiting on a reply from the team” [??] and then both a “response” and a “replay” [??] from the doctor herself. That’s when I finally realized “the team” was not about to answer my questions.
In exasperation, I rephrased my concerns into straightforward questions that should have been (but weren’t) addressed at the very first office visit: 1) what kind of cancer do I have, 2) what is the prognosis, and 3) what is the best way to treat it. I requested a reply from the doctor.
But once again “the team” caught the ball. This time they answered through “Mallory,” who has the unfortunate assignment of dealing with The Breast whenever I have had it up to here with bull****. She addressed the first question only: The Breast has no form of medullary disease, because the the pathology report issued by the University of Rochester is wrong.

Of course, she didn’t actually use the word “wrong” because no medical provider in her right mind would ever recognize, acknowledge, suggest, or admit to any error committed by another provider. I learned THAT lesson when Dr. Gandhi and “the team” erased my past medical history and review of systems, fearing that I might contaminate them with details they don’t like. In fact, that fear is precisely what eventuated this whole “don’t ask / don’t tell” thing, which frees the doctor and “the team” to create a sanitized, chart-worthy version of my health status and relegate me to a brainless gynoid blob called The Breast, who is not supposed to bother them by participating in her own health care.
Mallory knew she had to support both interpretations while categorically establishing the supremacy of Roswell’s. Following “our pathology review,” she wrote, “[i]t is possible that your previous oncologist/pathologist noted some medullary features/patterns[;] however[,] our team did not.”
Hmm. That would be pathologists. With an S. But that’s not important. What’s important is that I interpret her doublespeak correctly:
- Nobody is wrong.
- Everybody is right.
- But “our team” is righter.
Since the referenced “oncologist/pathologist[s]” are not on “our team,” their interpretation of the specimen simply doesn’t count. Whatever “features/patterns” these luckless outsiders observed must have defied the laws of physics and mutated into nothingness by the time the images were examined by a Roswell pathologist — but I question whether a Roswell pathologist was involved in any of this.

Shipra Gandhi, MD, above. I’m sure she’s very nice, but she doesn’t do appointments. That’s “team” work — but I have to pay doctor prices for it. From https://medicine.buffalo.edu/faculty/profile.html?ubit=shipraga
While completing my reply to Mallory, I was interrupted by a message from “Alison Courtney,” another member of “the team.” Her note was ostensibly conciliatory: “Of course it is reasonable to ask questions about your disease to better understand,” but we both knew that was a lie. Since the doctor doesn’t do phone calls (or email), Alison suggested I drive two hours to Buffalo to keep (and pay for) an appointment with Dr. Gandhi, and then drive two hours back home — with no assurance that the doctor would give me anything more “reasonable” than the rubbish “the team” had already supplied for free.

Alison Courtney, RN, above, who lacks the empathy (and intelligence) one would expect of a medical caregiver — the perfect choice for “the team.” From LinkedIn, https://www.linkedin.com/in/allison-courtney-aa5a63201/, December 29, 2023. Image no longer available.
Nevertheless, Alison continued to share her magnanimous good will: ”I know [she knows nothing] that navigating all of this information [what information? I wasn’t given any!] and managing this disease can be overwhelming [ditto the first comment], and I am sorry that you are going through this [she isn’t]. Thank you [for what?] and Happy New Year!”
What an arrogant way to slam the door — right in my face! Well, I suppose it’s a whole lot nicer than saying “don’t let it hitcha where the Good Lord splitcha,” even though that would have been much more considerate (and believable) than her feigned sympathy and phony good wishes.
I suppose it’s my own fault. The Breast should have known better. You know, “don’t ask/ don’t tell.” But despite the stress (I don’t do well with stupid) I did learn a lot. I learned that
1) I will never get any information from anyone at Roswell. They have put all questions — past, present, and future — permanently to rest once “the team” had shrewdly discovered and then, for some unknown reason, replaced the diagnostic findings in my prior records with one more to their liking. It was only under duress that “the team” reluctantly divulged their antithetical opinion and its supportive “documentation,” to wit:
an innocuous misimpression that had been blamelessly committed by no one, because the tissues were unstable and could not be trusted.
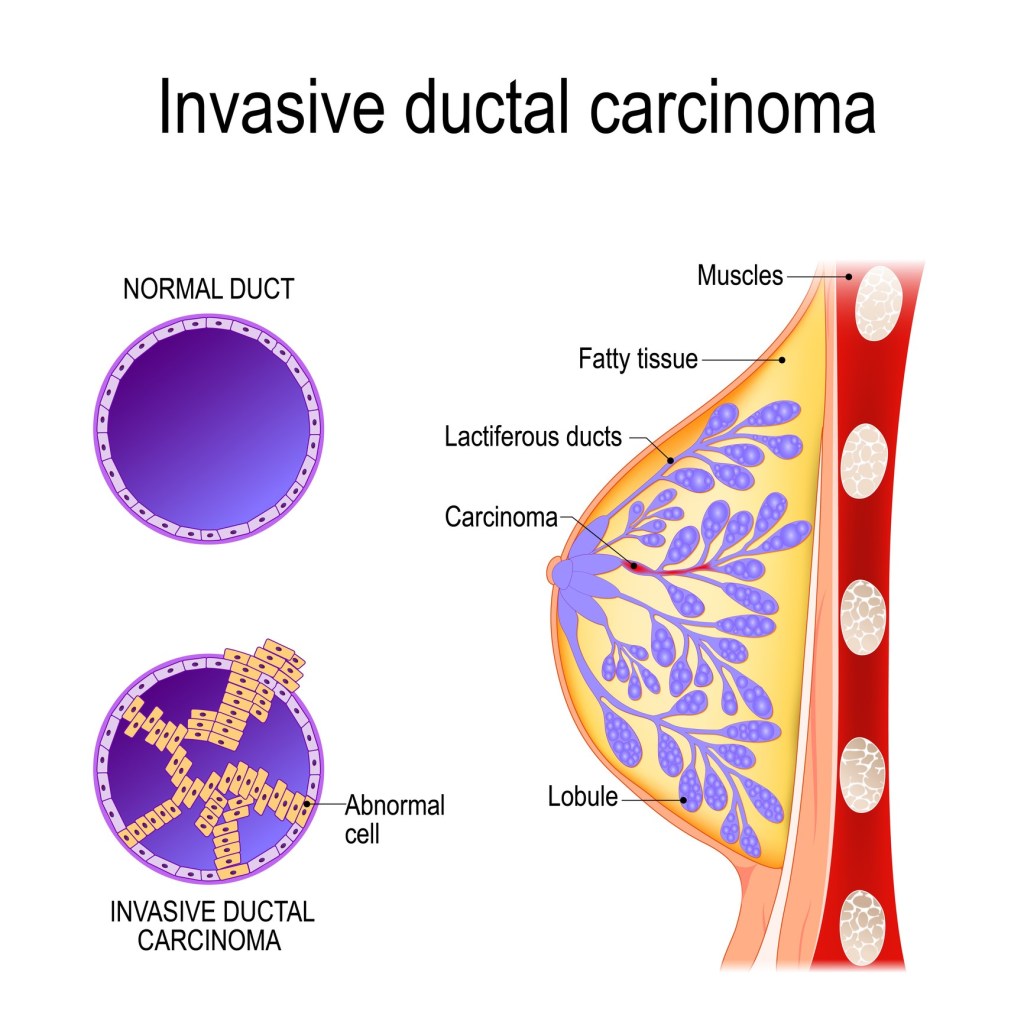
Invasive ductal carcinoma — but the cells must be examined by a pathologist to determine what kind of IDC it is. A “team” of nurses, even a Roswell “team,”is not qualified to examine and/or interpret pathologicl specimens.
2) Besides, The Breast has no business seeking such information. Much like Dr. Dhakal’s incompetence, this stuff is destined to remain under the silent control of Shipra Ghandi, MD and “our team.” And if The Breast continues to pursue the matter, it’s easy enough to dismiss her queries with a flippant “she has a bad relationship with her doctor.” It doesn’t matter if it’s with the doctor who nearly killed her or the one who hides behind “the team — or whether a “bad relationship” even exists at all — it doesn’t have to be true to be the perfect euphemism with which to label, blame, and then ignore The Breast. It just has to be charted, that’s all. They’ve done it before, and I have no doubt they will do it again ad nauseum.
Oh, look! TWO caregivers who want to protect Ajay Dhakal from himself by demanding I shut up! Holly Anderson, left, and Shipra Gandhi, center; From https://www.facebook.com/BreastCancerCoalitionofRochester.
Moreover,
3) I have a lot of damn nerve asking questions that require intelligent answers. Loosely quoting an appropriate sneer from Mel Brooks (“Blazing Saddles,” 1974): “Documentation? We don’t need no stinkin’ documentation.” Since it is an indisputable, black-letter-law fact that no medical provider ever makes a mistake that can’t be covered up, denied, hidden, manipulated, trivialized, reinterpreted, dismissed, and/or ignored, The Breast has a duty to believe whatever “our team” (and only “our team”) tells her to believe, even if it’s specious, incredulous, ridiculous, or dismissive. Especially if it’s specious, incredulous, ridiculous, or dismissive.
Alrighty then.
This leaves me no choice but to
3) flush any nascent trust down the toilet. I don’t need to know the dialectics; in fact, if I hadn’t been so persistent in pestering “the team” with gratuitous questions I never would have known that the conservation of matter doesn’t apply to my cancer-infested breast tissues. These unique and powerful cells of mine can transmogrify and even disappear idiopathically and at will — that is, until they are viewed by a Roswell pathologist. That’s when they suddenly become remarkably docile, nondescript, and whatever “our team” wants them to be.
But at this point I wonder if a Roswell pathologist was ever involved, because
4) As Mallory wrote, “our team” invalidated the UofR diagnosis after conducting a “pathology review.” However, my interactions with “[their] team” reveal it is comprised of a bunch of nurses and a PA or two, none of whom has ever demonstrated any kind of special training in pathology. So, I have no reason to doubt Mallory — this unreported and unsupported conclusion likely did originate from “the team,” because a board-certified pathologist would certainly have affirmed such important findings, which contradict those of two other board-certified pathologists (and a board-certified surgeon plus the board-certified physicians at Elizabeth Wende Breast Center), with a report or an addendum or a consultation note or something in writing to direct the plan of care. . .you know, like the EWBC and UofR physicians did. Their notes are available in my chart. . .but any such writings signed by a Roswell pathologist, Dr. Gandhi, or even “the team” are not.
But hey, there’s a bright side here. None of this will require life support — I’ve already been there, done that with Ajay Dhakal. Despite his ignorance and carelessness, I’m still here. . .wondering if my diagnosis is a guesstimate of what a couple of nurses or maybe a PA thinks I have, based on statistical proclivity (and Dr. Gandhi’s dictum) rather than expert interpretation of the tissues.
So, now that “the team” has severely but appropriately punished The Breast for her outrageous transgression of the treatment plan duly thunk up — not by a board-certified oncologist but by a medically uncertified Patient Advocate — I am tacitly expected to shut the f**k up (now, where have I heard THAT before, Holly Anderson). After all, I am damaged goods, courtesy of the ignorant Ajay Dhakal and the “don’t ask / don’t tell” medical strategy resulting therefrom. The Breast need not possess the intelligence required to understand her disease, she just needs to shut up. After all, it’s only for her own good. Besides, any further queries will just attract the same nonsense she’s already gotten and will risk pi$$ing off “the team” even further. Does The Breast really want them to slam the door in her face — again?

Apparently, it is whatever the Roswell Patient Advocate thinks it should be.
The standard of care followed by “the team” may be insulting, inappropriate, and humiliating, but it is not complicated: The Breast shows up to Roswell once every three months. At these visits she gets some blood work (but no CEA or any other appropriate cancer folllowup), and she can request a breast exam. That’s it. Full stop. Wham, bam, thank you ma’am. So simple (and useless) that it can be done in less than 5 minutes over the phone. The fact that this de minimus descendi care works best on women who don’t ask questions portends that future violations of “don’t ask / don’t tell” will not improve care but will indeed cause all kinds of absurdity and scorn to be heaped upon The Breast.
Just like it was on December 29.
I don’t like any of this. But I don’t have to like it. I just have to hope it works. . .until I realize that once again I’ve had it up to here with bull**** and start looking for an oncologist who treats his/her patients with respect. . .because Dr. Gandhi and her “team” apparently can’t or won’t do that.
Until then,
(but only until I find a good oncologist).
